Dr. Kevin Kunz speaking at the news conference, held by Zoom
(BIVN) – With Hawaiʻi island facing “an avalanche of overdoses (and) deaths” from the fentanyl epidemic, the Hawaiʻi Island Fentanyl Task Force is urging the community to make greater use of a medication, buprenorphine, in order to treat addiction.
Until January 12th, the Task Force says, the use of buprenorphine “was highly restricted due to archaic, regressive federal regulations.” However, “all of these restrictions have been lifted and now all medical providers can easily prescribe buprenorphine to appropriate patients with opioid use disorder.”
The Hawaiʻi Island Fentanyl Task Force was formed following the November 2021 death of a 14-year-old girl on Hawaiʻi island, in what was later confirmed to be a fentanyl overdose.
Fentanyl was first recognized on Hawaiʻi island in about 2017-18, the Task Force says. “Over the last 15 years fentanyl has become the leading cause of U.S. deaths in the age groups 18-45,” the coalition writes. “Federal data have indicated that there is now an overdose death every 11 days on Hawaii Island: the overwhelming majority of these involve fentanyl.”
During a news conference held over Zoom on Friday, Task Force lead Dr. C. Kimo Alameda introduced Dr. Kevin Kunz, who spoke on buprenorphine. Alameda also welcomed Amanda Deguair to the news conference. Deguair shared her own experiences with opioid addiction, and her recovery with the use of buprenorphine.
First, Dr. Kunz provided this commentary:
Buprenorphine, also known as Suboxone, Subutex and other brand names, is a safe and effective medication for opioid use disorder. Opioid Use Disorder – opioid addiction – is a brain disease that can develop with any exposure, repeat any exposure, to opioids. Opioids are obtained by prescription (like hydrocodone, oxycodone, and morphine) and illegal varieties are easily found on the street and the internet. Physicians and health care providers have had a significant barrier to prescribing buprenorphine, and the breakthrough is that these barriers have been removed. However, removing the arcane restrictions will not be enough.
Buprenorphine – bupe for short – is an FDA approved medications that eliminates both acute and chronic opioid drug withdrawal as well as drug craving. It has a 20 year researched and documented record of effectiveness. And now it can be easily prescribed by any medical provider.
The brain disease of addiction is often minimized in our society – many thought and some still think – that addiction is a moral, behavioral or legal issue. Addiction may precipitate these issues, yet it is primarily a disease. Just as diabetes and high blood pressure are diseases, so is addiction. Just as medications can help persons with diabetes and high blood pressure, so medications like buprenorphine can help persons with opioid use disorder stabilize and recover. This medication has been available on a highly restricted basis for over 20 years – and so it has not been in wide use. Only 1 in 10 people with any SUD receive evidence based treatment. Now that can change for those with OUD, especially now when we are being overwhelmed by the opioid and fentanyl epidemics.
The stigma and ignorance surrounding the disease of addiction is still limiting both society and the health care community from adopting this evidence based treatment. Opioid and fentanyl addiction had been viewed until 6 weeks ago as a primary criminal problem by our judicial systems and the U.S. Drug Enforcement Agency, the DEA. The DEA has now seen the light and believes that saving lives and getting treatment to those that need is a part of their mission. So on January 12 the disease all of the discriminatory and counter-productive federal regulations limiting prescriptions for buprenorphine was completely and totally rescinded.
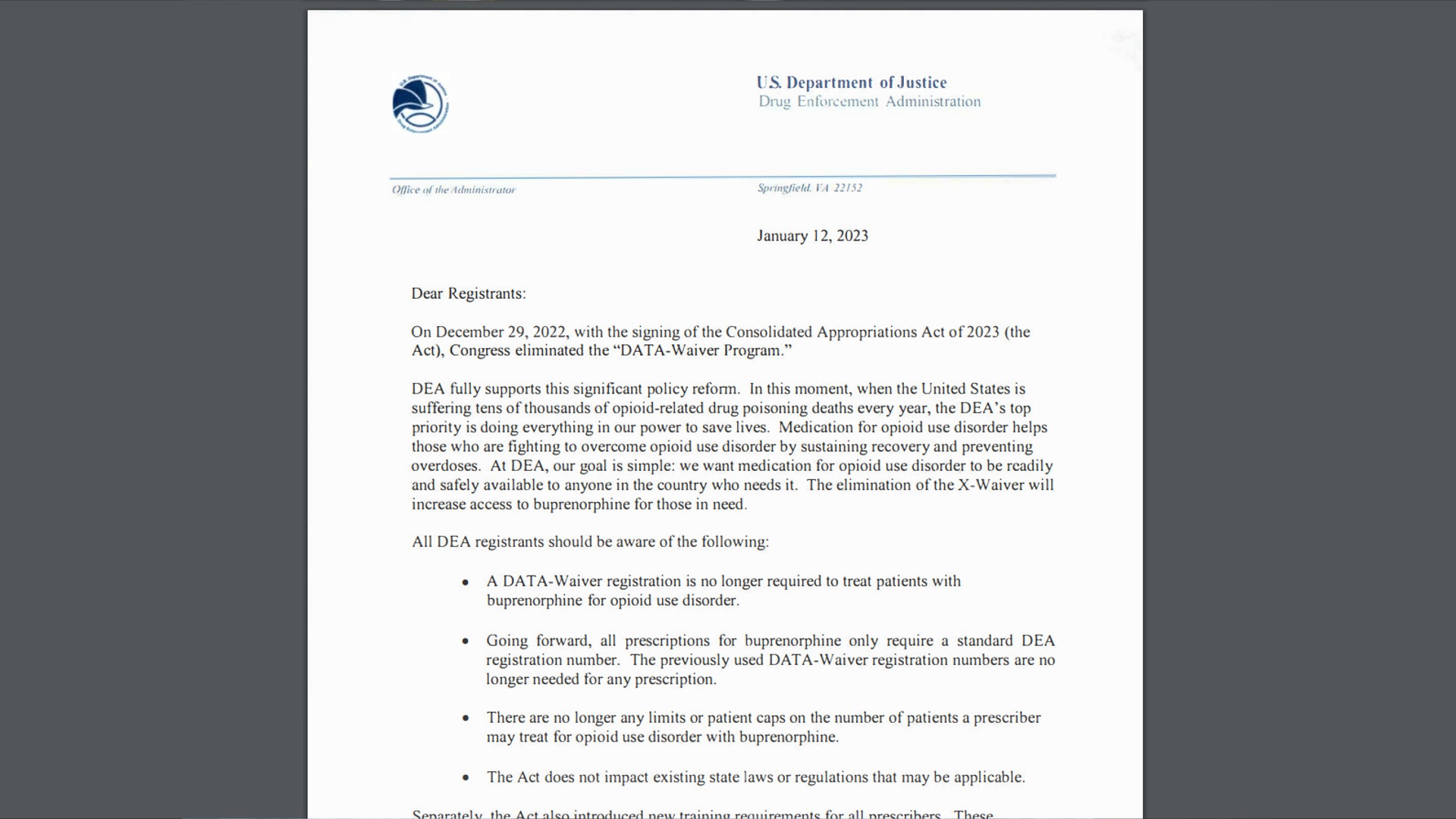
DEA letter provided by Hawaiʻi Island Fentanyl Task Force
The DEA gets it: this is a medical problem. So after 50 years, all parties agree that the war on drugs has not been effective, and that treatment is. All now agree, we will never incarcerate or bury our way out of the opioid epidemic. We are in a new era, and the new message is: Treatment works, it is available and recovery is possible.
Patients will tell us that Bupe has given them their lives back, and literally saved their lives. What does science say? This chart shows death rate comparisons in average persons, persons with OUD and persons with OUD prescribed buprenorphine. If you have OUD, you die at a rate 6 times higher than someone without OUD.
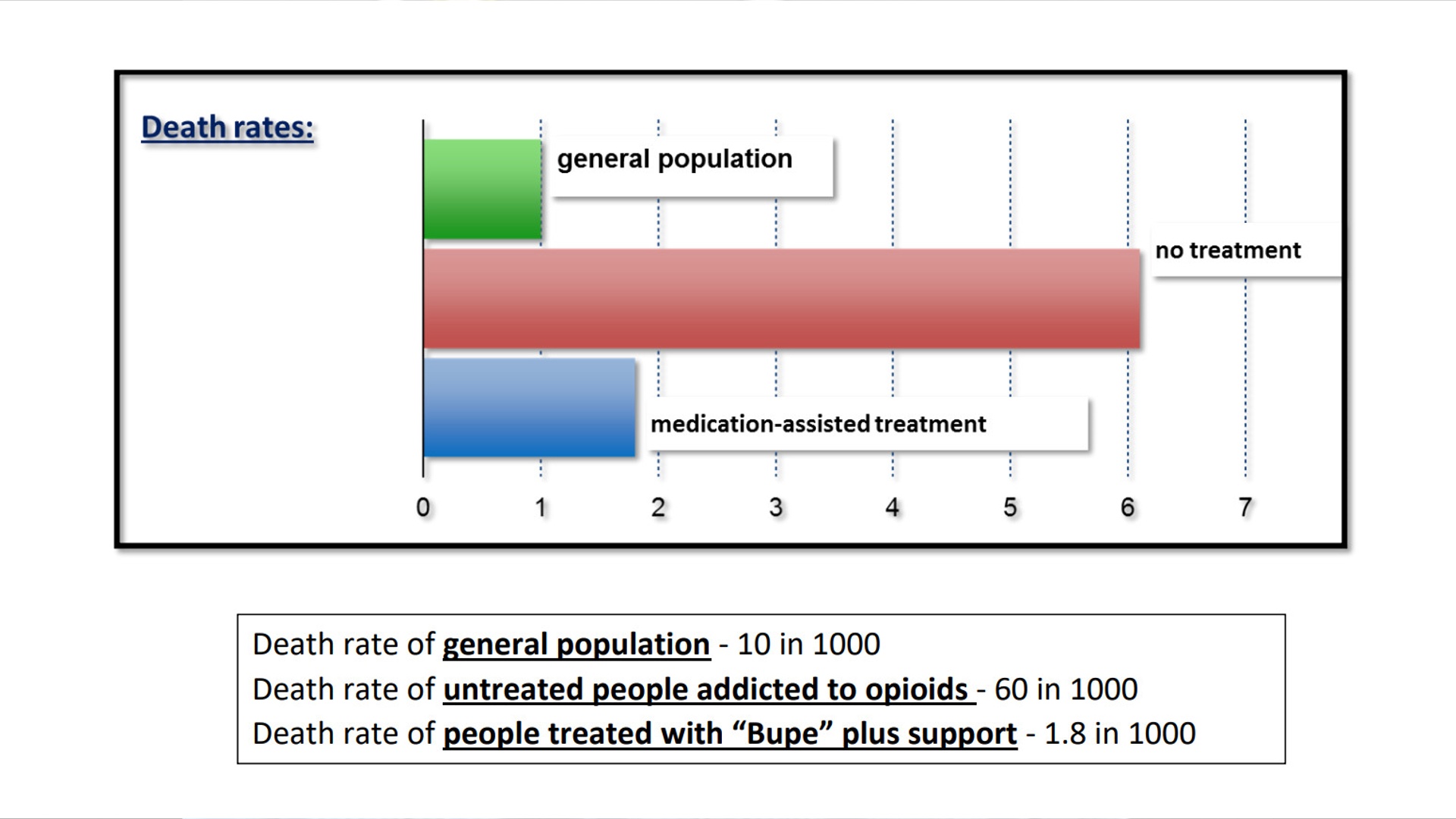
Graphic by the Hawaiʻi Island Fentanyl Task Force
As a community we must now address the significant remaining barriers in making this effective treatment available to Big Islanders in need. It is good news indeed that any medical provider in Hawaii can now prescribe. Yet they need encouragement and support to do so. Most do not know they can offer medication for opioid addiction. And many have fears about prescribing to people with addiction. Can you imagine if for any other disease there had been such restrictions? People with diabetes having no access to insulin? People with cancer not being prescribed medication that saves their lives? So our medical providers island wide need to step up. Many are already. They believe that it is their responsibility – their obligation – to be part of the solution, and to offer the gold-standard treatment to their patients. We are asking and encouraging all medical providers to answer this call: step up, do what only you can, write that prescription for Buprenorphine for your patients with OUD.
To address the human suffering and high social toll we have paid to the opioid crises, we must utilize all available means, as Dr. Alameda indicated on his chart. And today we call upon each of you, from every community sector who hears this message to step up. As Dr. Alameda noted, and something I must mention, is that there are two ways to reduce demand for addictive drugs: reduce the supply and reduce the demand. Hats off and Mahalo to the Big Island’s Hawaii Police Department – the work of our law enforcement officers has been incredible. They are true partners in this fight.
One key way we can reduce drug demand is by utilizing buprenorphine. We cannot let this medication sit in warehouses and in unopened pharmacy boxes while our children, our cousins, our neighbors die. The new reality is that every licensed physician, nurse practitioner or Physician Assistant can be part of the solution. People and families seeking help for the disease of opioid addiction can now access care from these nearly 500 medical providers on Hawaii Island – instead of a couple dozen – and over 5,000 medical providers statewide, instead of a few hundred. Let’s treat opioid use disorder like we treat other diseases: let’s start using the standard of care, and that includes the medication buprenorphine for OUD.
So we call out to all of you:
To physicians, physician assistants and advanced practice registered nurses: Ask your patients about their substance use. If they are using opioids problematically – either through prescriptions or an illicit supply- talks to them about buprenorphine. Consider prescribing it for them. You can help them get their life back, and help save their life. Their family, employers and community will also benefit.
Please don’t let fear cause you to stand on the sidelines. Don’t walk away because “it’s not worth the hassle”. You will find that your patients in recovery from addiction will give you a new view of your work.
It is not difficult to start a patient on this medication. There are easily accessible, brief one hour learning modules available on line. For instance, just Google “brief buprenorphine free training”. Contact us if you need more information.
To Hawaii medical, nursing, social work and other health training institutions: please make sure your students and your residents are knowledgeable and skilled in identifying and treating opioid use disorder. I recently met a graduate who just finished 7 years of professional training – yet he had no reasonable current concept of addiction or its treatment. Preventing and treating addiction are as important, if not more important than the treatment of other routinely seen illnesses. And more rewarding.
To Hawaii’s insurance companies: HMSA, Kaiser, United Health Care, Ohana Health Care, and others: remove the barriers of “pre-authorization” and prescribing limits you place on this medication. It is ironic that providers can easily prescribe opioid medications that are potentially addictive, yet have barriers prescribing effective medications like buprenorphine for treatment of opioid use disorder. Back off. Do the right thing. It will save you money and it will save and restore lives.
To all of Hawaii’s pharmacies and corporate owners: Longs-CVS, Walmart, Costco, Safeway and others – please adequately stock buprenorphine. And please treat these patients as you would treat your patients with any other disease. Reduce the stigma of addiction. Remember that this medication is as effective as insulin for diabetes. Addiction is a disease like any other: no one plans to get it. Remove your barriers to accessing buprenorphine. Treat these patients as you would any patient.
To hospitals and hospital emergency rooms: Emergency rooms are the front line of the opioid crisis. Thank you for the work you do. As providers in this setting, every day you see persons with OUD, often in a crisis mode when they may be open to help. Now you can start them on this safe and effective medication and refer them back to their community provider – then the patient’s own primary care provider can refill the prescription. It is a new world for Emergency Department physicians: you no longer have any of the numerous restrictions that previously discouraged the prescribing of buprenorphine.
To substance use treatment programs, psychologists, social workers, therapists and counselors: If you are treating persons with opioid addiction, suggest buprenorphine to them as an element in the standard of care, adding to the behavioral and cognitive therapies you deliver. Keep in mind that “Together is better”: counseling plus medication. In fact, the Gold Standard for treating opioid use disorder is the combination of medication and support, such as counseling, or participation in a community mutual help group, such as Narcotics Anonymous, Alcoholics Anonymous, Celebrate Recovery or others. Buprenorphine will stabilize the brain disease of addiction. And allow counseling or group participation to be more effective. It’s hard to load new brain software for living, if the hardware of the brain is out of order. Work with and refer your patients with OUD to their primary care providers for information and treatment with buprenorphine.
To Mayor Roth: Mahalo for your initial and continuing support for the Hawaii Island Fentanyl Task Force. You and your leadership team have helped give a voice where there was silence. To Governor Green: Mahalo for your years of leadership and your clinical work on the Big Island. You know all too well the crisis we are having. With your leadership, the Department of Health, and all state agencies can effectively address this crisis which is raining acid on the heart of our community and our state.
To persons already in recovery: Congratulations on your recovery and the work you have done. You know that addiction can be a chronic disease and it needs long term attention. You know what it takes to stand up against this disease, and to be open for help. If you know someone struggling with opioid addiction, remember that there are many paths to recovery. Know that taking a medication like buprenorphine is not trading one drug for another. This medication does not promote euphoria or a drug high. It takes away craving and withdrawal. It saves lives. Let your experience lead others to a path out of addiction.
To families struggling with an opioid addicted member, and especially those families who have lost a loved one to opioid overdose: Thank you for standing up. Thank you for having the courage to turn your grief into advocacy for prevention and treatment. You are a voice that will be heard. You honor your loved ones by sharing your story and helping others avoid the tragedy you have suffered.
Finally, to those of you struggling with opioid addiction: You are a good person with a bad disease. It has kidnapped you. It has brought you to places and to feelings unimaginable. You may think you are alone or that very few without this condition could understand your situation. We know it has hurt your sense of self; it has hurt your relations with all who you love, and all who love you. It has changed your life for the worst.
Please know that treatment is available.
Don’t give up.
Treatment works.
Recovery is possible.
Here is a transcript of the emotional, personal story shared by Amanda Deguair:
Aloha, My name is Amanda Deguair It is not easy to come here and be this open in front of everyone, but if this can reach one person who is addicted and feels as if there’s no way out, I’m here to tell you that there is. and I was asked to be part of this coalition fight against the Opioid Crisis that we are faced with on the Big Island. I believe it will take all of us, those in recovery, family members, co-workers, and especially those in the medical field to help our community. Even if you don’t know anyone personally who struggles with this chronic disease, we all are affected. We need a community solution. I am a recovered addict and my life is amazing today.
I grew up in a home with good values, love, and support. We all don’t come from troubled backgrounds filled with trauma.
I began like most, sneaking cigarettes around the age of 11, then I had my first “real drink” in the 7th grade. I clearly remember that night, going to a party with older kids, full of fear. “Will anyone like me? Do I look okay? What do I say?” and something magically happened when I took that first drink. I felt like I belonged there and all those fears were gone.
By High School, I was dabbling with drugs with other drugs.. My friend group began to change and I sought out people who partied like I did. I thought this was what kids do, we experiment. By my 20’s, Drinking and drugging was just a part of life. But inside, I felt like I was starting to spin out of control. And this is when I began experiencing back problems, so the doctor prescribed me Vicodin. I soon began seeking out doctors who would give me more and more.
Amanda Deguair, speaking at the news conference, held over Zoom
At 24, I got pregnant with my first child and during the first 2yrs of his life, I was becoming the parent I never wanted to be. All I ever wanted to be my whole life was to be a mother. Here I had everything I could ever hope for. Had you asked me, I would have told you I would lay my life down for my child, and any mom would say the same. The problem is, addiction doesn’t care about you or the people you love., it doesn’t care about your children.
I wanted a better life for my son and I, so I found my way into a recovery community. I figured if I could remove the alcohol and hard drugs, life would improve, I didn’t see the Vicodin being a problem, I mean, they came from a “Doctor” and I had a legitimate reason for taking them.
During my first years in recovery, I got married , I had 2 more children, and I was doing all I could to manage the pills and trying to be in recovery, only knowing deep down inside that I was a hypocrite because I was addicted to Vicodin. The more I tried to control the opioids, the worse it got. I then ended up with a spinal fusion and I felt even more justified to continue taking them. The snowball effect was unbelievable.
At this point I had been on Vicodin for 10yrs, I can’t begin to tell you the fear that someone feels with the thought of giving up Opioids. The fear of withdrawal and the fear of always wanting and needing them. It’s paralyzing. I thought “I can’t do anything without my pills?” “I can’t get through a day without them?” I knew the pills made me “normal” and the fear of never feeling “normal” was crippling.
My “Ah-ha” moment was on a Thursday night around 5pm. I had all 3 of the kids in the car and it was just around sunset, a beautiful time of the day in Kona. Everything I had ever wanted was in that car and they were all happy. They were singing and laughing, it was the moment that any mother could ever ask for. The problem was, I was running out of pills and would not have enough to last through the weekend. My brain was racing on what to do. Should I look online or somewhere else? I have been caught at every pharmacy, trying to fill my prescription too early, and they were onto my game, so where can I go? The kids laughter and noise made me angry because my mind was racing. It was the moment I knew that I was so wrapped in addiction, because nothing else mattered. Those 3 kids in the car didn’t matter. I didn’t want to continue living like this, I knew I needed help. I missed so many joyful moments due to my addiction. So I went home and finally got honest with my husband and I started looking for help. I think that fear of withdrawal is the biggest reason most of us stay in addiction. I thought I was going to have to suffer to get better, and I didn’t think I would survive that.
So I found one of the few doctors on the Big Island who offered Suboxone. The Bup plan was clearly spelled out. I was led into an exam room and when my withdrawal was sufficient but not severe, I was given a tab of suboxone to put under my tongue. About 30 mins later, when the doctor returned, he turned the light on, and couldn’t believe it! I felt more normal than I’d felt in 10yrs!. I had walked into that office, terrified, craving a pill and my mind was racing. And within 30 mins, I felt like the fight was over and there was hope again. I also didn’t feel “high”. To not feel “high” and to not be craving a pill was unbelievable. Had I known what I was going to experience, I wouldn’t have waited so long. I want to thank that doctor for not shaming me and making me feel like a “drug addict”, in the sense that I was a bad person. He treated me with dignity and respect and that made getting help so much easier. I hope others find an understanding medical provider to help them live a new life as I did. Now that suboxone is more readily available to anyone who needs it, this is possible.
Since then, I’ve had some major medical issues. I have a rare brain condition called Arnold chiari Malformation and I deal with chronic pain daily, Had it not been for Bup, I definitely would have picked up the other opioids again. Subox takes care of my addiction and my chronic pain and allows me to live a life in recovery
For myself, I couldn’t do Suboxone only, I had to immerse myself in a recovery group and live life with the support of a fellowship.
Today I stand here with 18yrs of recovery . This is a progressive disease, and I know today, had I not been given suboxone, , I would not be standing here and my children would be without a mother. My hope for today is that one person might hear this and will feel comfortable to reach out to get help. and that those who are in a position to help, which is all of you, understand that we are not bad people, we are people who have a disease and we need help, not judgment or criticism. Recovery and a normal life is possible.

by Big Island Video News
on at
STORY SUMMARY
HILO, Hawaiʻi - Experts are urging the community to normalize the use of buprenorphine as an effective treatment for opioid/fentanyl addiction.